Save 15% on select classes!





Craniosacral Therapy and Myofascial Release
Powerful In Person Training Classes for Healthcare Professionals

Meet Steve Heinrich, PT — a nationally respected instructor who blends deep expertise with humility, humor, and heart.
Full Certification Program - Multiple Options
Why Learn with Steve
With over forty years in private practice, hospital rehabilitation, and home health leadership, Steve brings real-world experience to every seminar through powerful stories and practical clinical insight. He has spent decades teaching Craniosacral Therapy (CST) and Myofascial Release (MFR), creating engaging, hands-on courses that are both inspiring and immediately applicable to your practice.
A Unified CST + MFR Approach
Steve presents CST and MFR as two inseparable parts of one integrated system: CST focuses on the environment of the brain and spinal cord, while MFR addresses the body’s soft tissues. Both are taught as whole-person, mind–body approaches centered on listening, seeing the bigger picture, and removing barriers to healing in a safe, honest, non-toxic therapeutic relationship.
Structure First, Then Subtle Listening
What sets Steve apart is his insistence on first mastering anatomy, structure, function, and balance of the craniosacral and fascial systems before “just listening” to the body. He believes that true clinical artistry comes only after knowing the rules well enough to bend them safely and effectively, giving students both confidence and clarity in their touch and decision-making.
Grounded, Not Vague
Although he respects biodynamic models and has personally benefited from them, Steve has found that approaches taught without a solid structural foundation often leave clinicians unable to explain or reproduce their results. Drawing on more than thirty years of studying osteopathic and structural principles, he teaches CST and MFR in a way that is both deeply skilled and clearly explainable, so students know what they are feeling, why it matters, and how to refine it.
Choosing The Right Teacher
Steve encourages practitioners to choose instructors who teach from love, acceptance, and genuinely low ego, rather than personality or mystique. His seminars are built around humility, safety, and service, creating a learning environment where questions are welcomed, hands-on practice is prioritized, and each participant feels supported as they grow their skills and expand their therapeutic impact.
My Personal View and Teaching Approach
I believe CST and MFR are best seen as two parts of one whole—intimately connected but with a slightly different focus and different time frames and pressures, as they are dealing with two separate but connected systems. CST deals with the environment of the brain and spinal cord, and MFR deals with the soft tissue—but both are about listening and looking at the bigger picture, connecting with the patient in an honest and non-toxic way, and looking for the blocks to healing whether they are in the tissue or in the mind-body connection.
The main difference in how I teach CST and MFR compared to others is that I want students to understand the function, structure, and balance of both the craniosacral and fascial systems first before they “just listen” to the system—as I often say, “You need to know the rules before you break the rules.”
I know several excellent therapists who follow the biodynamic model, and I have had truly amazing personal experiences being treated by these therapists. However, when I ask them how they did what they did, or what they were doing specifically, they couldn’t tell me.
Unfortunately, from what I can see, practitioners who go straight into BCST without the structural background are missing a lot of the pieces. I believe that what I do at my level is very much this kind of work, but I have been studying the structure and the osteopathic foundational materials for over thirty years. I know what the function, structure, and optimal balance of the two systems look and feel like, and I want to approach my treatment and teaching from that focus.
How to Choose a Teacher and Approach
The main thing to watch out for when learning CST and MFR is the ego of the teacher and the approach—it needs to come from a place of love and acceptance and low ego for the best results. My personal bias is that the best approach to the entire subject is to understand and fully integrate the structure and foundational materials as the basis for this complex, intriguing, and ultimately life-changing work.
So: “How do you eat an elephant?” “One bite at a time.” But… it is a big elephant!
Keep Learning
Advance your skills with hands-on Craniosacral Therapy and Myofascial Release classes Seminars Northwest
Upcoming Classes
Hands-on classes to deepen your healing skills.


Craniosacral Therapy I Lewiston, Idaho - Twin Rivers Therapeutic Massage Academy March 28 & 29, 2026 Contact Jolene Ross, LMT 208-290-2409 or Joleneross1966@gmail.com
Myofascial Release I Calgary, Alberta March 18, 19, 2026 Seminars for Health - https://www.seminarsforhealthcourses.com/
Myofascial Release II Calgary, Alberta March 20 & 21, 2026 Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy III Lewiston, Idaho - Twin Rivers Therapeutic Massage Academy April 11 & 12, 2026 Contact Jolene Ross, LMT 208-290-2409 or Joleneross1966@gmail.com
Craniosacral Therapy I Missoula, Montana - April 18 & 19, 2026 Contact- Sacred Roots Massage School https://www.massageschoolofmontana.com/
Craniosacral Therapy I Calgary, Alberta May 13 &14, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy II Calgary, Alberta May 15 &16, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy III Calgary, Alberta May 18 &19, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
These classes are not your ordinary continuing education fare. They tend to be peak life learning events that change lives and career trajectories! Steve Heinrich, PT
Craniosacral Therapy II Edmonton, Alberta September 20 & 21, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy III Edmonton, Alberta September 22 & 23, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Myofascial Release I Edmonton, Alberta September 24 & 25, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy I Post Falls, Idaho - October 10 & 11, 2026 American Institute of Clinical Massage Contact Steve Heinrich, PT 208-691-0310 or
Craniosacral Therapy I Calgary, Alberta October 21 & 22, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy II Calgary, Alberta October 23 & 24, 2026 Contact - Seminars for Health - https://www.seminarsforhealthcourses.com/
Craniosacral Therapy I Port Townsend, Washington - December 12 & 13, 2026 Port Townsend School of Massage Contact Steve Heinrich, PT 208-691-0310 or
Seminars Northwest and Steve Heinrich, PT teach classes with several great organizations.
Classes highlighted in blue require you to contact these organizations directly to register. See contact information for specifics.
Classes highlighted in green are available on this website for registration.
Welcome to Seminars Northwest
Empowering therapists with hands-on classes in craniosacral therapy, myofascial release, and essential skills.


150+
15
Trusted for Quality Education
5 stars
Seminars Northwest
Training the best clinicians for over thirty years
Hands-on classes to deepen your healing skills and knowledge.
Craniosacral Therapy I - II - III
Learn masterful techniques to balance the Craniosacral system for profound gentle healing.
Myofascial Release I - II
Master Myofascial Release Develop Transformative Soft Tissue Pain Management Skills
Boost your abilities with practical, skill-building workshops. Become fully certified in CST and MFR!
Skills Development




Full Certification Program - Multiple Options
Get in Touch
Questions about classes? We're here to help you grow your skills.
Phone
208-691-0310
Moments from our hands-on therapy and skills workshops.









Meet the Instructor - Steve Heinrich, PT Thirty Years of Teaching Experience
Success Stories!
Good Morning Steve,
I just wanted to share another success story. I have been seeing a client for 10yrs and she has always had horrible low back pain and sciatica. I have been able to keep her at a tolerable pain and movement level over those years. Thursday she came in and was in extreme pain and is getting ready to start on a trip to California to see family. I did some myofascial work on her and it was getting better, then I did a dural tube release and the direction of energy technique between the hands on her low back. She said the tingling in her toes was going away and by the end of the treatment she was much better. 20 minutes later she texted me and said "What was that stuff called that you did to me?" She is out of pain and feeling great.
Great Job Jolene!! Love it and keep up the good work!!!

CST and MFR
Myodural Bridge Function and Cranial Base Release – CST Perspective
Role of the Myodural Bridge
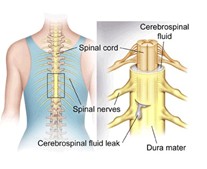
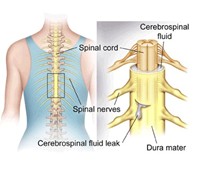
The myodural bridge (MDB) links the deep suboccipital muscles to the cervical dura, helping stabilize the dural tube so it does not buckle, fold, or slacken with head and neck movement. When these muscles become tight, asymmetric, or overactive, abnormal tension can be transmitted to the dura and may contribute to headaches that radiate toward the temples, eyes, or forehead.
MDB, CSF Dynamics, and Symptoms
The MDB appears to contribute to cerebrospinal fluid (CSF) movement by transmitting rhythmic mechanical forces from suboccipital muscle activity into the dural system, functioning like a subtle pump for CSF circulation. When those muscles are in spasm, fatigued, or poorly coordinated, CSF flow around the cranio cervical junction can become reduced or irregular, and patients often describe pressure at the base of the skull, mental fogginess, dizziness, headaches with bending forward, and worsening symptoms during Valsalva, coughing, or rapid position changes—patterns that are consistent with MDB related dysfunction.
Proprioception, Oculomotor Control, and MDB Dysfunction
The MDB also participates in sensorimotor control by linking cervical proprioception with eye and head movement, balance mechanisms, and brainstem sensory processing. Disturbance in this system often coexists with chronic dizziness, motion sensitivity, visual convergence strain, vestibular mismatch, autonomic symptoms, upper cervical instability, and headaches that can follow concussion or whiplash, since traumatic loading of the cranio cervical junction frequently stresses the MDB and its associated musculature.
Mechanisms of Injury and Chronicity
Acceleration–deceleration injuries, sports impacts, repetitive micro strain, prolonged forward head posture, or long term protective muscle guarding can overload the MDB and its muscular attachments. Over time, this may lead to persistent or recurrent symptoms that respond poorly to standard approaches focused only on muscles, joints, or medications and do not address dural tension or cranio cervical mechanics.
CST Cranial Base Release Approach
To improve MDB function and reduce headache and related symptoms, a craniosacral therapy (CST) protocol can be used that emphasizes cranial base work and CSF optimization. A typical sequence may include multiple prolonged CV4 type still points to encourage CSF function, followed by cranial base release; then balancing of the sphenoid and sphenobasilar synchondrosis; assessment and correction of maxillary dysfunction at the sphenoid; release of the vomer and ethmoid; followed by a second cranial base release and a final CV4 still point. This sequence aims to decompress the neurocranium from the Viscerocranium, improve cranio cervical alignment, enhance dural mobility, and support more efficient CSF flow, which can lessen referred pain into the head and face. Many individuals report a distinct sensation of decompression or lightness in the suboccipital region during or shortly after treatment.
Patients Who May Benefit
This MDB focused CST approach may be appropriate for patients with one or more of the following:
• Chronic cervicogenic headaches or “pressure” at the skull base.
• Migraines associated with neck tension or upper cervical stiffness.
• Dizziness, motion or visual sensitivity, or post concussion symptoms.
• Persistent brain fog, difficulty tolerating head movement, or visual strain.
• Suspected atlas/upper cervical instability, history of whiplash, or symptoms aggravated by poor posture, prolonged screen use, or looking down at phones.
Conclusion:
In individuals whose headaches or migraines have not responded adequately to typical medication based management, evaluation of the myodural bridge and a CST oriented cranial base release protocol may provide a useful missing component of care
Steve Heinrich PT


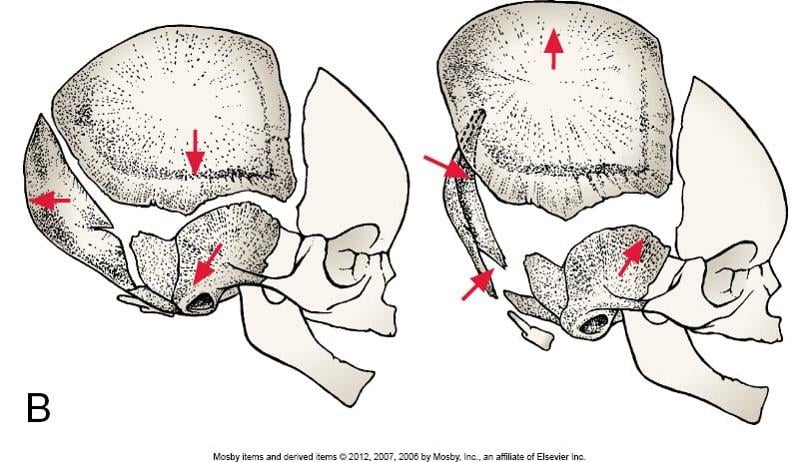
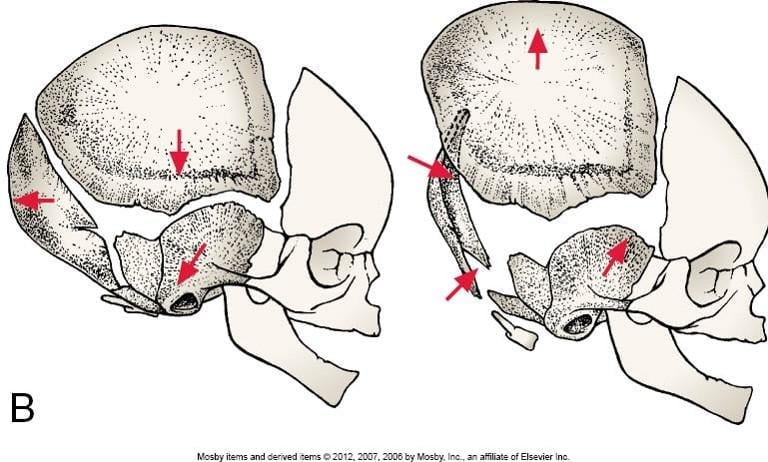
Balancing the Palatine Bones
Steve Heinrich, PT
Often overlooked by craniosacral therapists, balancing or decompressing the palatine bones can have profound positive effects for patients with facial pain, headaches, sinus pressure, eustachian tube congestion, tinnitus and infections of the mastoid portion of the temporal bone. This was recently reinforced for me when a patient came in for severe Mastoiditis. The patient sought me out because “Steve does weird things with heads…” and they were desperate to avoid surgery when antibiotics didn’t resolve the infection.
Treatment is very straightforward but as noted above, often overlooked due to the location of the palatine bones, their proximity to the gag reflex at the back of the palate and therapist’s reluctance to do intraoral work.
I typically do an ear pull along with the palatine release, unwinding the tentorial membranes and releasing the eustachian tube simultaneously. This time, gently compressing and decompressing the patients left palatine bone – do both sides with very gentle pressure – typically less than five grams – I felt a strong vibration under my finger as it interrogated the palatine bone followed by a loud, clearly audible ‘click or pop’ as the palatine bone decompressed. The patient felt a rushing sensation in her sinuses and hard palate along with an awareness of draining, heat and a release of pressure in, around and behind her left ear. Releasing the palatine bone allowed the infection to drain, her ear to clear and most importantly to her, her symptoms nearly immediately resolved, and she avoided having major surgery to remove a large portion of her left temporal bone.
It’s easy to overlook the palatines but sometimes it is critical to take a second look at these cranial restrictions and treat them with direct compression / decompression techniques combined with ear pulls and still points at the maxilla, even if your reputation isn’t for doing “weird things with heads…”
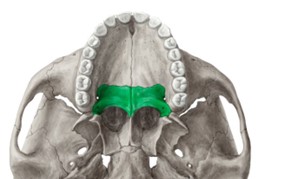
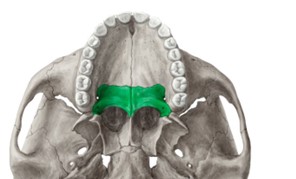
Key Features & Anatomical Relations
The palatine bones are a pair of L-shaped bones found along the posterior aspects of the nasal and oral cavities. They are classified as irregular bones and contribute to the formation of the nasal cavities, bony hard palate and the Viscerocranium.
Mastoiditis is an infection or inflammation of the mastoid bone, which is located behind the ear and is part of the temporal bone. The mastoid bone has a honeycomb-like structure with air spaces called mastoid cells that help maintain the middle ear's air space. Mastoiditis can occur when a middle ear infection, such as otitis media, spreads to the mastoid bone and infects or inflames the mastoid cells.
https://www.elsevier.com/.../axial.../palatine-bone/17739
https://my.clevelandclinic.org/.../dise.../24469-mastoiditis
CST and MFR


Dycum and the Dural Tube
Brian was twenty-three, had two young children, was married and starting to live his best life when a tree fell and struck him in the back while logging. Fortunately, it was a small tree and not one of the widow maker varieties that take out so many loggers in the northwest each year. I had known Brian from another logging injury the year before and he was a likable, very cheerful young man that everyone liked on sight. He was full of youth and vigor and his smile was enough to light up a room, so when I saw him walking into my office, bent over to nearly 90 degrees and with the haggard expression of a much older man, I was alarmed. When Brian told me the story of the accident and resulting injuries leading to multiple disk ruptures and complicated neurosurgery, I could not help but feel sad, and even worse, angry, when he added the comment, “And my surgeon says that he’s done everything he can and I just have to live this way.”
Brian was in severe pain, could not stand upright and his spine was bent at nearly 90 degrees with cervical hyperextension so that he could see where he was walking. The only semi comfortable position for him was in a recliner with his knees drawn up and a pillow behind his neck - some of you can see where this is going already.
On further questioning, Brian - not his real name – said, “Oh and the surgeon said that my dural tube was torn in the accident.” I looked at his back and he had a very small scar at T10 – it had now been over six months since his surgery and it was well healed – and it was so small the tight that I almost overlooked it. Brian was nearly in tears, he said, “I’ve got two kids, my wife is working two jobs, I can’t work, what am I going to do? I can’t live this way.” I felt like crying too, and I wondered what I could possibly do to help, but almost on instinct I said something very rash that I have questioned nearly every day over the twenty plus years since then. I said, “Brian, we are not going to let this stand.” And in foolishness, optimism, or desperation, I went into the storeroom and got a piece of blue Dycum, the sticky plastic material occupational therapists often use to assist arthritis patients grip objects and came back to the treatment room.
My assistant Kathy and I piled up several pillows and Brian lay over the table with the pillows supporting his trunk and his feet on the floor. Kathy got onto the other side of the table and gently pulled Brian’s head forward out of hyperextension until he felt a pull in his scar and I grasped the scar with the Dycum and we began to do a dural tube release, slowly with 5 grams of pressure.
Incredibly, the scar began to unwind and within a few minutes, Brian told us that his headache that he’d had ever since the injury, was lessening. We continued to release the Dural tube for about twenty minutes and Brian started to sweat and pant, but as his pain was decreasing, we continued, although with very light pressure.
At the twenty-minute mark, I asked Brian to stand up, and he stood with only about thirty degrees of flexion, a neutral cervical spine, and a reported seventy percent reduction in pain. We could not believe our eyes. Brian came back for two more sessions and we repeated the gentle Dural tube release using his scar for one handle and the Occiput for another and within a total of three sessions he was upright, had full mobility of his spine and all the pain was gone.
I now speculate that the tear in the Dura had scarred down and was putting a low grade but constant pull on the Dural tube which Brian tried to accommodate by flexing his spine and extending his neck, all in an unconscious attempt to find relief, which just fed more slack to the scar which, tentacle like, kept pulling and adapting and taking up any slack, locking down the Occiput and flexing the spine. A Dural tube release and Dycum was able to unwind that scar and give Brian back enough flex in his system to move freely and get out of pain. I have since seen Brian with his wife and kids, and every time I see him, he gives me a hug and I can see a sparkle back in his eyes. Incidentally, he quit the woods, went back to school, and now makes his living far from falling trees.
‘There are more things in heaven and earth, Horatio, than are dreamt of in your philosophy’ Hamlet, Act 1, Scene 5
I was teaching a class near Seattle a few years ago when a quite amazing thing happened to me. It was during a break in class and one of the students came up and asked me to demonstrate one of the techniques we were discussing, which I was happy to do. I asked her to lie on the table and I started to demonstrate, I think it was a parietal lift technique, when suddenly it was as if I were no longer in the classroom, no longer near Seattle or the Pacific Northwest at all. I felt literally, in every sense of the term, somewhere else. I was standing in a clearing in a jungle, moats of light lit the bamboo forest and I could smell the earthy loam and hear with utmost clarity the calls of birds and other jungle creatures. Then, I heard an almost infrasonic sound, a low rumbling growl and felt every hair on the back of my neck stand up. Looking around I saw, winding sinuously through the bamboo stalks, a huge Bengal Tiger so real that I could see flecks of saliva on its whiskers and flakes of yellow pollen shining on its sleek striped pelt. It paused for a long second and stared deeply into my eyes, then without another sound, it stepped right through me becoming smoke and leaving me shaking.
I believe I was seeing my student’s spirit, her soul essence, so to speak, and I was both shaken and honored by the experience.
The Frontal Lift
Jane was in tears as she told me the story of her injury. Partially because she felt responsible for her accident, I believe, and partially – maybe the far bigger part - because her neurologist told her it was all in her head. Unfortunately, that seems to be far too common in our world, “I can’t figure it out, the tests and MRI’s are negative, so it must be in your head.” Jane was frustrated because she had seen her family physician, a chiropractor, two other physical therapists and a neurologist, none of which had done anything to solve her problems which were severe headaches resulting from a bonk on the head – for which she felt responsible. It was a toxic combination of factors and as I listened to her story, it resulted in tears of frustration and anger.
It was snowing and Jane wore glasses so she’d put on a long billed cap to shield her lenses from the snow as she walked from her car to the gym where she worked out. Thirty-six, tall and willowy, Jane was the prototypical gym attendee, and for six months, she hadn’t been able to work out or do much of anything because of the pain. Walking in to the gym that snowy morning, Jane had veered to the right of the pathway to allow two other women to pass and walked head first into a low overhanging beam that held up the portico. Jane hit her head, fell and embarrassed herself in front of her peers, felt ashamed and incensed over the “It’s all in your head” comment from the neurologist and angry at the many thousands of dollars she had spent trying to correct the situation when someone told her to “Go see Steve, he does weird things with heads…” A familiar refrain I have heard about my work for many years.
I listened in silence as Jane relayed her story, feeling frustrated with the neurologist and wanting to help but not sure, anything I could do would make a difference after all the tests and specialists had come up with nothing. Nevertheless, taking a deep breath I asked Jane to lay down on the table and starting with the capstone of the cranial vault, the frontal bone – like one of those wooden puzzles where you have to find the piece that moves first before you can unlock it – I began to do a frontal compression decompression technique.
Following the frontal bone down into compression it sank like an elevator on greased rails for several seconds before beginning to twist counterclockwise, then lower on the right, followed by the left until I felt the frontal bone seat or stop compressing. Jane hadn’t said anything since she had lain down but as I began to lift the frontal bone back up decompressing it she let out a great sigh and even more tears started to fall. Knowing not to quit, I continued to lift the frontal bone with classic light pressure and it unwound like a little UFO floating up toward the ceiling.
About half way through the frontal lift, Jane let out an even bigger sigh and said - this still gives me goose bumps – “It feels like you are pouring a pitcher of light inside my head.” As I lifted, the frontal bone, connected into the Falx Cerebri began to unwind releasing what must have been scar tissue that resulted from the trauma of striking her head – and I surmise -causing a micro tear of the Falx that didn’t show up on MRI. As I lifted, the scar tissue released and the pain began to dissipate. Jane left my office feeling 80% better and was fully out of pain permanently in three sessions.
While Jane’s results were the most dramatic, I have treated hundreds of other patients who responded similarly to CST following trauma to the head from car accidents, flying baseball and soccer balls as well and trips, slips and falls, punches and martial arts.
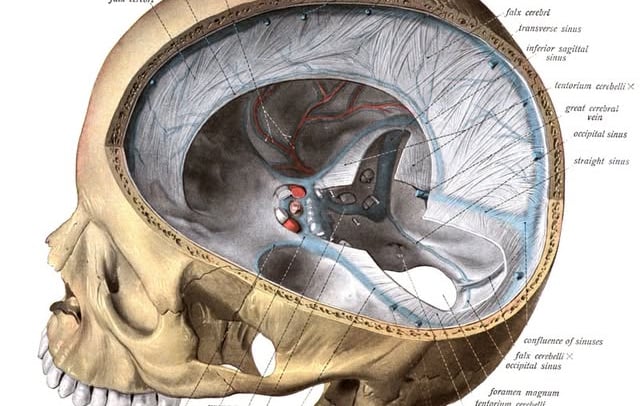
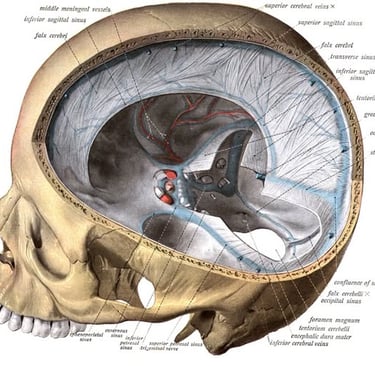
I don’t pretend to know the exact mechanism of the release of scar tissue, or even if that was really what the problem was but it is what I believe happened, based on the results of treatment and looking at many fresh cadaver images which show apparent scar tissue adaptations and areas of ischemic, tight membranes of the Falx and the Tentorum which are the result of the insidious and compressive forces of scar tissue. My first job following PT school was in a burn and trauma center and I can tell you from firsthand experience about the force and pain produced by scar tissue, so I am not surprised that scars in the Falx and Tentourm would produce pain as well.
I typically follow this pattern when doing CST Releases – Frontal bone compression decompression, Parietal bone compression decompression, Sphenoid compression decompression and lateral / side bending assessment and treatment, Sphenobasilar synchondrosis assessment and treatment, Temporal bone assessment, Cranial base release and Dural tube release. Still points and assessment of the CSR also included. I hope this helps and that fewer patients will hear, “It’s all in your head,” from anyone.
Craniosacral Therapy and Migraine Headaches
A few years ago, I decided to keep a log of the cranial lesion patterns of patients who sought treatment for Migraine Headaches. I was thinking of writing a paper but never got around to it, however, I did keep track of the cranial lesion patterns of twenty nine patients – not a big enough sample to draw firm conclusions but enough to see some interesting patterns. Migraines are a complex subject with many components not related to cranial dysfunction and I do not purport to be an expert those aspects, but this is what I found. [i]Twenty-three patients had a lateral strain lesion of the sphenoid, of which nineteen were right lateral lesion patterns. Eighteen had cranial base compression with anterior head position and adaptive muscle shortening,[ii]and all of the twenty-three patients with sphenoid strain patterns, had some degree of concomitant sphenobasilar synchondrosis dysfunction.
Balancing the sphenoid and the sphenobasilar synchondrosis, along with releasing the cranial base restriction resulted in a patient reported - roughly 75 - 80% reduction in the frequency and intensity of migraine headaches. I tried to keep in touch with the study group for up to a year but that proved impractical and I lost track of over half of the study group within six months. This sample is too small, it was observed by only one therapist and ultimately I didn’t think I could write a defensible paper about it, but my findings were interesting and consistent across the sample. I haven’t read any research papers focusing on this aspect of treatment so I don’t know who else has studied this but whenever I see a patient that has migraines, I always check for sphenoid lesions, sphenobasilar synchondrosis dysfunction and cranial base issues. Thoughts?
[i] Twenty-nine total patients in the sample, twenty-four female, five male.
[ii] I blamed keyboards and computers at the time and it can only have gotten worse with all the mobile tech out there
Go see Steve; he does weird things with heads…
This is the way I have been addressed for more than thirty years now, ever since taking my first CST and MFR classes. Maybe it’s my fault for not articulating what I do with more accuracy or style or something…. But there you go, thirty plus years of ‘he does weird things with heads.’ I was working in the rehabilitation department of our local hospital one afternoon when I received a very strange phone call from a pediatrician I know, and he opened with a new version of that statement. “Hi, this is Dr Jones, and I’m not exactly sure what you do, but I hear you do things with heads… and well, we had a little guy born last night that had a really tough time and we had to use forceps, and well, could you give it a look?”
I have a philosophy, probably born of my background in private practice, never to say no but to try to accommodate and asses, so I told Dr Jones I’d be right up to the neonatal ward and see what I could do. Arriving in the ward, I was happy to find that the patient’s mother was a previous patient and she was happy to see me. I oohed and aahed over the little baby while inwardly cringing at the sight that lay sleeping peacefully in the little plastic bassinette. My patient and his poor mother had been through a war. Not only was his head traumatized from the forceps, his little head was a more pronounced version of the Saturday Night Live, Cone head character, because his head had a nearly thirty-degree cant to the side, so cone head with a twist.
I had no idea what to do and cursing inwardly at what had been done to this little child, I sat down next to the bassinette and chatted with the mother for a second while I thought what to do next. I reasoned that if anything could help, it would be to start with the sphenoid, so with my arm resting on the rim of the bassinette, I reached down and extremely lightly picked up the sphenoid and began a classic sphenoid lift, reasoning that surely it did not need any more compression.
Now, this is the most bizarre thing that has ever happened to me in a career filled with bizarre happenings. It is irrational, confusing, and amazing, and even now, many years later it makes the hair stand up on the back of my neck. I was not watching what I was doing, but chatting lightly with the mother while praying that I could help this little child and doubting myself at every other word, when a shock went through my right arm so strongly that I thought two things simultaneously: One, that I had somehow been electrocuted, and Two, that the kid had bit me. I knew he was only a few hours old and that he had no teeth, but the sensation was so sharp and strong that I jerked my hand back and looked down at the still sleeping baby in anticipation of burns or a missing digit even though I was nowhere near his mouth, and instead saw to my utter amazement a perfectly round little head and an expression of complete peace on the now fully straightened face.
Lifting the sphenoid, the master bone of the cranial system, the entire skull had snapped back into position with such force and power that it generated a piezoelectric shock of amazing physical and perhaps spiritual power that left the baby whole and the therapist shattered. The mother and I looked at the sleeping baby in awe and grinning a stupid grin, I almost whooped in happiness to see this miracle, this wonder.
I was walking down the street at lunch a few days later and saw my patient and his mother coming out of a store and stopped to once again ooh and aawh over the little baby, this time with genuine admiration and joy, for there before me, wrapped in a colorful fleece blanket was ‘my baby’ as cute and button eyed as you would expect with a perfectly round little head and a beautiful life ahead of him.
I am truly blessed to have stumbled onto CST and MFR as a young therapist and now, many years later having practiced and taught nearly every day for over thirty years, I am more powerfully convinced of its transformative beauty than ever, and I can still feel that surge of electricity going up my arm as I write this now. Cary on, even in the face of self-doubt, be gentle, be kind, leave the ego out of it and let Spirit work through your hands and amazing things will happen.